Eye and Vision Items
Items 8, 17.b., 18.d, 31-34, 50-54: Index to Ocular and Visual Parts of FAA Pilot Medical Exam & History
Apr 2014
Abbreviated Briefing:
Overview of the Eye and Vision parts of the FAA Guidelines.
Because visual perception is so critical to aviation, the FAA has devised complex and highly structured components of the pilot medical exam devoted to the eyes and vision. There is a dedicated history component (item 18.d) plus 10 separate exam areas and 8 sections of medical flight test (MFT) description.
The process begins with Medical history--personal information provided by the applicant or other doctors who submit this information through the AME on the applicant's behalf. Starting with Item 18.d (Eye or vision trouble except glasses), this is a yes/no attestation on the FAA Form 8500-8 which is filled out in advance through the FAA MedXPress system. If "yes" is indicated, details must be provided and these elaborations will be discussed with the AME at time of the exam. The AME will inquire about changes in vision, unusual visual experiences (halos, scintillations, etc.), sensitivity to light, injuries, surgery, or current use of medication
The exam portion represents objective data that the AME collects and discovers through clinical inspection and testing. Items 31-34 are components listed in the observable "eye" sub-section, and all of these areas will be checked by the doctor during the flight physical. Items 50-54 are located in the demonstrable "vision" sub-section. Vision components will be assessed by the doctor or a technician through various performance tests such as the familiar eye charts and color vision testing equipment. Although there is some overlap, the eye portion is roughly an assessment of anatomy (structure), and the vision portions are measurements of physiology (function).
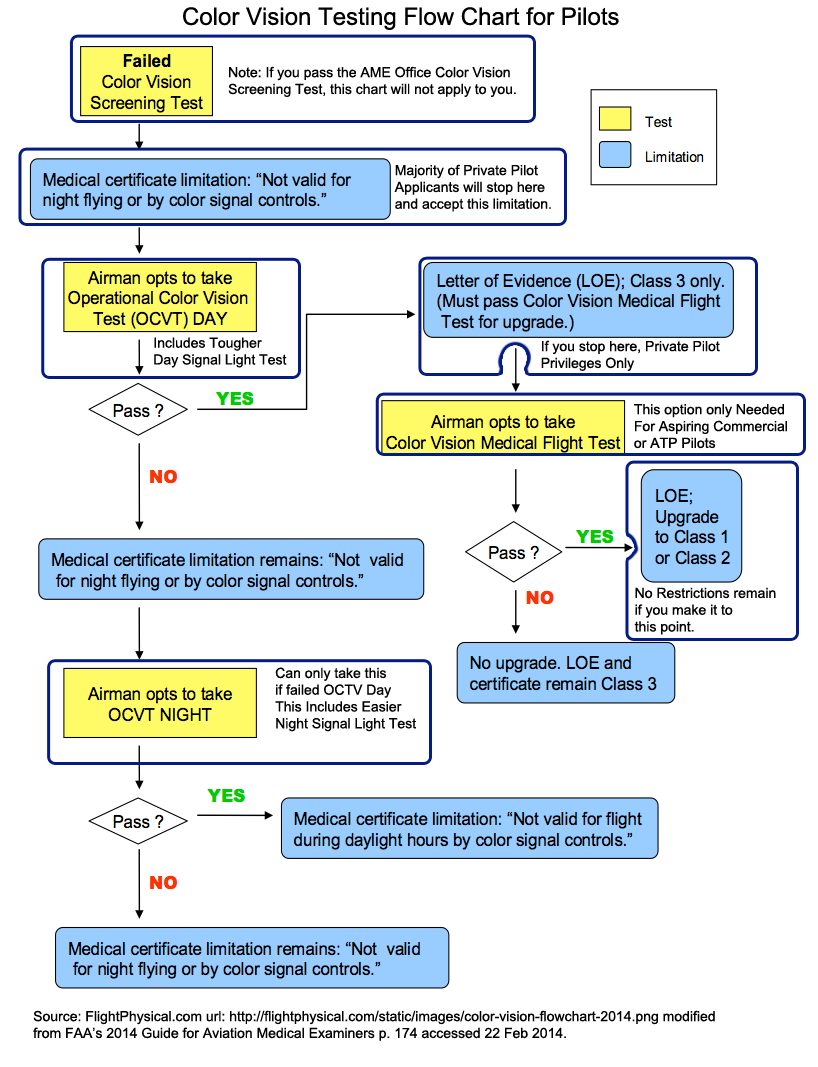
Also included below are links to the color vision flow chart which graphically describes options for applicants who fail the office color vision test but still want to acquire or maintain a pilot certificate. Finally, there are several pages dedicated to the special Medical Flight Test (MFT) process for aspiring pilots with only one eye or pilot applicants who have difficulty with color discrimination (color blind pilots). Most pilots will not need to take an MFT, but these more extensive (and expensive) medical certification options are available for pilot applicants with specific problems who are interested in demonstrating their ability to function while airborne but cannot otherwise pass the in-office eye and vision screening tests.
{kind=link}
Advertisement
Guidance is compiled and interpreted by professional pilots and physicians at FlightPhysical.com from the 2014 AME Guide pages 53-65, FAA and FDA web data (www.FAA.gov & www.FDA.gov), instructions specified in the Aeronautical Information Manual, Federal Air Surgeon Bulletins from 1999-2015, and 14 CFR Part 61 and Part 67 (the FARs).
I. Code of Federal Regulations (Legal Source)
For Overall Guidance for all classes, refer to: 14 CFR 67.103(e), 67.203(e), and 67.303(d):
No acute or chronic pathological condition of either the eye or adnexa that interferes with the proper function of the eye, that may reasonably be expected to progress to that degree, or that may reasonably be expected to be aggravated by flying.
For Specific Legal Guidance, you may refer to the actual legal code as stratified below by Class of Pilot Medical Certificate
-
First Class Standards 14 CFR 67.103
-
Second-Class Standards 14 CFR 67.203
-
Third-Class Standards 14 CFR 67.303
For practical, non-legal guidelines on the clinical exam techniques, the sections below are helpful to AMEs and pilots alike. These instructions are paraphrased from the 2014 AME Guide which is a useful interpretive manual provided by the FAA.
AME Examination Techniques
During the eye examination, your AME checks for diseases or defects that may cause a failure in visual function while flying or pain sufficient to interfere with safely performing airman duties. Tell your AME about any changes in vision, unusual visual experiences (halos, scintillations, etc.), sensitivity to light, injuries, surgery, or current use of medication. Report inordinate difficulties with eye fatigue or strain ort any history of serious eye disease such as glaucoma or other diseases commonly associated with secondary eye changes, such as diabetes.
The AME will consider the following clinical signs during the eye exam:
-
External Inspection:
- Color — redness or suffusion of allergy, drug use, glaucoma, infection, trauma, jaundice, ciliary flush of Iritis, and the green or brown Kayser-Fleischer Ring of Wilson's disease.
- Swelling — abscess, allergy, cyst, exophthalmos, myxedema, or tumor.
- Other — clarity, discharge, dryness, ptosis, protosis, spasm (tic), tropion, or ulcer.
-
Ophthalmoscopic examination. AMEs each develop their own routines for ophthalmoscopic examinations to aid in the conduct of a comprehensive eye assessment. The FAA states that routine use of a mydriatic (dilating drops) is not recommended.
- Cornea — observe for abrasions, calcium deposits, contact lenses, dystrophy, keratoconus, pterygium, scars, or ulceration. Contact lenses should be removed several hours before examination of the eye. (See Item 50, Distant Vision)
- Pupils and Iris — check for the presence of synechiae and uveitis. Size, shape, and reaction to light should be evaluated during the ophthalmoscopic examination. Observe for coloboma, reaction to light, or disparity in size.
- Aqueous — hyphema or iridocyclitis.
- Lens — observe for aphakia, discoloration, dislocation, cataract, or an implanted lens.
- Vitreous — note discoloration, hyaloid artery, floaters, or strands.
- Optic nerve — observe for atrophy, hemorrhage, cupping, or papilledema.
- Retina and choroid — examine for evidence of coloboma, choroiditis, detachment of the retina, diabetic retinopathy, retinitis, retinitis pigmentosa, retinal tumor, macular or other degeneration, toxoplasmosis, etc.
- Ocular Motility. Motility may be assessed by having the applicant follow a point light source with both eyes, the Examiner moving the light into right and left upper and lower quadrants while observing the individual and the conjugate motions of each eye. The Examiner then brings the light to center front and advances it toward the nose observing for convergence. End point nystagmus is a physiologic nystagmus and is not considered to be significant. It need not be reported. (For further consideration of nystagmus, see Item 50., Distant Vision.)
- Monocular Vision. An applicant will be considered monocular when there is only one eye or when the best corrected distant visual acuity in the poorer eye is no better than 20/200. An individual with one eye, or effective visual acuity equivalent to monocular, may be considered for medical certification, any class, through the special issuance section of part 67 (14 CFR 67.401). In amblyopia ex anopsia, the visual acuity loss is simply recorded in Item 50 of FAA Form 8500-8, and visual standards are applied as usual. If the standards are not met, a Report of Eye Evaluation, FAA Form 8500-7, should be submitted for consideration. Although it has been repeatedly demonstrated that binocular vision is not a prerequisite for flying, some aspects of depth perception, either by stereopsis or by monocular cues, are necessary. It takes time for the monocular airman to develop the techniques to interpret the monocular cues that substitute for stereopsis; such as, the interposition of objects, convergence, geometrical perspective, distribution of light and shade, size of known objects, aerial perspective, and motion parallax. In addition, it takes time for the monocular airman to compensate for his or her decrease in effective visual field. A monocular airman’s effective visual field is reduced by as much as 30% by monocularity. This is especially important because of speed smear; i.e., the effect of speed diminishes the effective visual field such that normal visual field is decreased from 180 degrees to as narrow as 42 degrees or less as speed increases. A monocular airman’s reduced effective visual field would be reduced even further than 42 degrees by speed smear.
-
Contact Lenses. The use of contact lens(es) for monovision correction is not allowed:
- The use of a contact lens in one eye for near vision and in the other eye for distant vision is not acceptable (for example: pilots with myopia plus presbyopia).
- The use of a contact lens in one eye for near vision and the use of no contact lens in the other eye is not acceptable (for example: pilots with presbyopia but no myopia).
Additionally, designer contact lenses that introduce color (tinted lenses), restrict the field of vision, or significantly diminish transmitted light are not allowed.
FAA note: the use of binocular contact lenses for distance-correction-only is acceptable. In this instance, no special evaluation or SODA is routinely required for a distance-vision-only contact lens wearer who meets the standard and has no complications. Binocular bifocal or binocular multifocal contact lenses are acceptable under the Protocol for Binocular Multifocal and Accommodating Devices .
- Intraocular Devices. Binocular airman using multifocal or accommodating ophthalmic devices may be issued an airman medical certificate in accordance with the Protocol for Binocular Multifocal and Accommodating Devices.
- Orthokeratology (Ortho-K) is the use of rigid gas-permeable contact lenses, normally worn only during sleep, to improve vision through reshaping of the cornea. It is used as an alternative to eyeglasses, refractive surgery, or for those who prefer not to wear contact lenses while awake. The correction is not permanent and visual acuity can regress while not wearing the Ortho-K lenses. There is no reasonable or reliable way to determine standards for the entire period the lenses are removed. Therefore, to be found qualified, applicants who use Ortho-K lenses must meet the applicable vision standard while wearing the Ortho-K lenses AND must wear the Ortho-K lenses while piloting aircraft. The limitation “must use Ortho-K lenses while performing pilot duties” must be placed on the medical certificate.
-
Glaucoma. The Examiner should deny or defer issuance of a medical certificate to an applicant if there is a loss of visual fields, a significant change in visual acuity, or newly diagnosed intraocular hypertension.
The FAA may grant an Authorization under the special issuance section of Part 67 (14 CFR 67.401) on an individual basis. The Examiner must obtain a report of Ophthalmological Evaluation for Glaucoma (FAA Form 8500-14) from an ophthalmologist. See Glaucoma Worksheet. Because secondary glaucoma is caused by known pathology such as; uveitis or trauma, eligibility must largely depend upon that pathology. Secondary glaucoma is often unilateral, and if the cause or disease process is no longer active and the other eye remains normal certification is likely.
Applicants with primary or secondary narrow angle glaucoma are usually denied because of the risk of an attack of angle closure, because of incapacitating symptoms of severe pain, nausea, transitory loss of accommodative power, blurred vision, halos, epiphora, or iridoparesis. Central venous occlusion can occur with catastrophic loss of vision. However, when surgery such as iridectomy or iridencleisis has been performed satisfactorily more than 3 months before the application, the likelihood of difficulties is considerably more remote, and applicants in that situation may be favorably considered.
An applicant with unilateral or bilateral open angle glaucoma may be certified by the FAA (with follow-up required) when a current ophthalmological report substantiates that pressures are under adequate control, there is little or no visual field loss or other complications, and the person tolerates small to moderate doses of allowable medications. Individuals who have had filter surgery for their glaucoma, or combined glaucoma/cataract surgery, can be considered when stable and without complications. A few applicants have been certified following their demonstration of adequate control with oral medication. Neither miotics nor mydriatics are necessarily medically disqualifying.
However, miotics such as pilocarpine cause pupillary constriction and could conceivably interfere with night vision. Although the FAA no longer routinely prohibits pilots who use such medications from flying at night, it may be worthwhile for the Examiner to discuss this aspect of the use of miotics with applicants. If considerable disturbance in night vision is documented, the FAA may limit the medical certificate: NOT VALID FOR NIGHT FLYING
- Sunglasses. Sunglasses are not acceptable as the only means of correction to meet visual standards, but may be used for backup purposes if they provide the necessary correction. Airmen should be encouraged to use sunglasses in bright daylight but must be cautioned that, under conditions of low illumination, they may compromise vision. Mention should be made that sunglasses do not protect the eyes from the effects of ultra violet radiation without special glass or coatings and that photosensitive lenses are unsuitable for aviation purposes because they respond to changes in light intensity too slowly. The so-called "blue blockers" may not be suitable since they block the blue light used in many current panel displays. Polarized sunglasses are unacceptable if the windscreen is also polarized.
-
Refractive Procedures. The FAA accepts the following Food and Drug Administration approved refractive procedures for visual acuity correction:
- Radial Keratotomy (RK)
- Epikeratophakia
- Laser-Assisted In Situ Keratomileusis (LASIK), including Wavefront-guided LASIK
- Photorefractive Keratectomy (PRK)
- Conductive Keratoplasty (CK)
The FAA realizes that these procedures have potential adverse effects that could be incompatible with flying duties. Potential side effects include corneal scarring or opacities. Other concerns include worsening or variability of vision over time and night-glare.
The FAA expects that airmen will not resume airman duties until their treating health care professional determines that their post-operative vision has stabilized, there are no significant adverse effects or complications (such as halos, rings, haze, impaired night vision and glare), the appropriate vision standards are met, and reviewed by an Examiner or AMCD. When this determination is made, the airman should have the treating health care professional document this in the health care record, a copy of which should be forwarded to the AMCD before resumption of airman duties. If the health care professional's determination is favorable, the applicant may resume airman duties, after consultation and review by an Examiner, unless informed otherwise by the FAA.
An applicant treated with a refractive procedure may be issued a medical certificate by the Examiner if the applicant meets the visual acuity standards and the Report of Eye Evaluation (FAA Form 8500-7) indicates that healing is complete; visual acuity remains stable; and the applicant does not suffer sequela such as; glare intolerance, halos, rings, impaired night vision, or any other complications. There should be no other pathology of the affected eye(s). If the procedure was done 2 years ago or longer, the FAA may accept the Examiner's eye evaluation and an airman statement regarding the absence of adverse sequela.
If the procedure was performed within the last 2 years, the airman must provide a report to the AMCD from the treating health care professional to document the date of procedure, any adverse effects or complications, and when the airman returned to flying duties. If the report is favorable and the airman meets the
appropriate vision standards, the applicant may resume airman duties, unless informed otherwise by the FAA.
Conductive Keratoplasty (CK): CK is used for correction of farsightedness. As this procedure is not considered permanent and there is expected regression of visual acuity in time, the FAA may grant an Authorization for special issuance of a medical certificate under 14 CFR 67.401 to an applicant who has had CK. The FAA evaluates CK procedures on an individual basis following a waiting period of 6 months. The waiting period is required to permit adequate adjustment period for fluctuating visual acuity. The Examiner can facilitate FAA review by obtaining all pre- and post-operative medical records, a Report of Eye Evaluation (FAA Form 8500-7) from a treating or evaluating eye specialist with comment regarding any adverse effects or complications related to the procedure.
Related Pages:
Medical History Related to the Eye
- 8. Eye Color (For Identification)
- 17.b. Contact Lenses (for Near Vision)
- 18.d. Eye or vision trouble except glasses
Anatomy (Eye Structure)
Physiology (Visual Function)
- 50. Distant Vision
- 51.a. Near Vision
- 51.b. Intermediate Vision
- 52. Color Vision
- 53. Field of Vision
- 54. Heterophoria
Medical Flight Tests for those with Waiverable Vision Defects
- Medical Flight Tests Overview
- Medical Flight Tests General Instructions
- Decision Flow Chart for Pilots Who Fail Color Vision Test (Graphic)
- Medical Flight Tests Procedures
- Color Vision Flight Test
- Medical Flight Tests: Signal Light Test
- Medical Flight Tests: Monocular Vision (for pilots with vision in a single eye )
- Operational Color Vision Test (OCVT)
This page discussed the Eyes & Vision section of the Fight Physical Examination required of pilots.
Reminder: use FlightPhysical.com to familiarize yourself with aviation medical regulations and guidelines, but always discuss your specific situation with one or more AMEs before dedicating resources toward expensive clinical workups. Find an AME now